Aortadissectie
Aortadissectie
Auteur: J. Sprakel, MD - Laatste update: 14-06-2014
Aortadissectie
Oorzaak
- - Scheur in de wand van de aorta, de zogenaamde entry, waardoor naast het "ware" lumen een "vals" lumen ontstaat, hierbij kunnen 3 dingen gebeuren:
1. Bloed in valse lumen kan distaal weer terugkeren in het oorspronkelijke (ware) lumen ("re-entry")
2. Bloed in valse lumen kan ware lumen dichtdrukken → acute ischemie van organen distaal van occlusie
3. Ruptuur van aorta - - Prevalentie van 2-4 per 100.000 inwoners 1
- - Ratio: ♂ : ♀ = 3 : 1
- - Leeftijd: 35-85 jaar, piek 50-65 jaar
Kliniek
Symptomen
- - Zeer intense, scheurende pijn tussen de schouderbladen 2
- - Uitstraling naar schouder, nek, arm, kaak, abdomen en heupen
- - Soms pijn verschuivend naar distaal bij progressie dissectie
- - Soms symptomen passende bij infarct door dissectieflap in arterie (hart, hersenen, nieren, darmen)
- - Nausea, diaphorese (zweten), vomitus
- - Collaps
- - Doodsangst
Risicofactoren
- - Hypertensie
- - Erfelijke bindweefselziekten (M. Marfan, Ehler-Danlos type IV)
- - Congenitale cardiovasculaire abnormaliteiten
- - Atherosclerose (t.g.v. roken, hypercholesterolaemie)
- - Granulomateuze arteritis
- - (Hoog energetische) trauma
- - Zwangerschap
- - Turner syndroom
- - Metabole afwijkingen
- - Cocaïne gebruik (crack)
- - Iatrogeen (CAG, chirurgie)
Lichamelijk onderzoek
- - Polsdeficit
- - Hypertensie met links-rechts verschil
- - AoI geruis (2/3de bij de proximale dissecties)
- - Perifere tekenen AoI
- - Decompensatio cordis (zelden)
- - Effusie linker pleuraholte
- - Harttamponade
- - Neurologische complicaties
- CVA
- Paresthesieën
- Syndroom v. Horner - - Nierfalen
Diagnostiek
- - ABG met lactaat
- - Lab: Lichte leukocytose, anemie, ASAT en CK normaal, LDH evt. verhoogd
- - ECG: meestal normaal, tenzij myocardinfarct wordt veroorzaakt door dissectie
- - X-thorax: in 90% verwijde thoracale aorta, bulge in aortacontour, pleurale efussie linker thoraxhelft
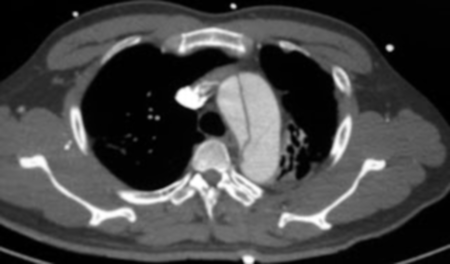
- - CT-a: gouden standaard (sensitiviteit >90%, specificiteit > 85%)
- - MRI: beste non-invasieve manier (sensitiviteit en specificiteit bijna 100%) , echter vaak niet goed mogelijk bij dissectiepatiënten i.v.m. lang stilliggen
- - Echo cor bij type A dissectie (doet aortaklep mee?)
Classificatie
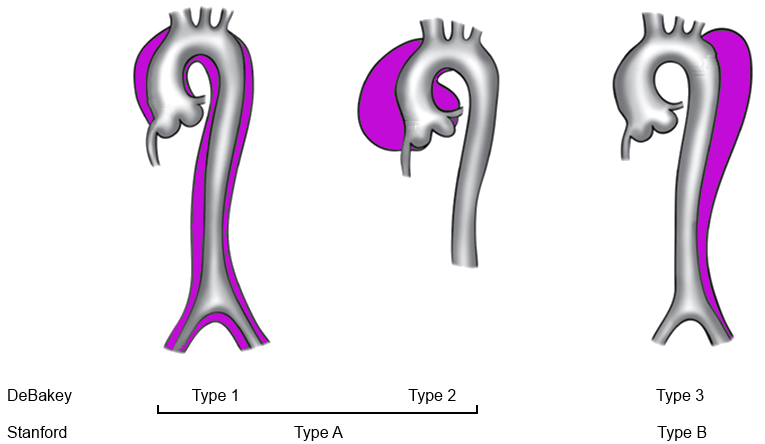
- - Stanford classificatie 3
- Type A: begint bij aortaklep
- Type B: begint vanaf a. subclavia sinistra - - DeBakey classificatie 4
- Type 1: begint bij aortaklep, reikend voorbij de halsvaten
- Type 2: begint bij aortaklep, reikend tot de halsvaten
- Type 3: begint vanaf a. subclavia sinistra - - Acuut vs Chronisch 5
Acuut: Diagnose gesteld binnen 2 weken na het ontstaan klachten
Chronisch: Diagnose gesteld > 2 weken na het ontstaan klachten - - Ongecompliceerd vs gecompliceerd 6,7
Gecompliceerd:
- Onbehandelbare hypertensie of onbehandelbare pijn
- Snelle toename diameter aorta tpv dissectie (>1 cm binnen enige weken)
- Ruptuur of een dreigende ruptuur
- Orgaanischemie
Conservatieve behandeling
- Indicaties:
- - Ongecompliceerde aortadissectie Stanford type B
- Behandeling
- - Opname IC of CCU voor strikte bloeddrukregulatie waarbij systolische bloeddruk < 120 mmHg 5
- - Pijnstilling
- - Lange termijn behandeling: Beta-blokkade of calcium antagonist in combinatie met antihypertensiva (ACE-inhibitor)
- Follow-up
- - Policontrole na 1, 3, 6 en 12 maanden, daarna jaarlijks
- - Follow-up beeldvorming middels MRI
- - Aandachtspunten tijdens follow-up: tekenen van aorta expansie, aneurysmaformatie, tekenen van lekkages op anastomoseplaatsen en stents, malperfusie
Operatieve behandeling
- Indicaties:
- - Gecompliceerde aortadissectie Stanford type B
- - Stanford type A
- Behandeling
- Gecompliceerde aortadissectie Stanford type B
- - Endovasculaire stent-graft in de thoracale aorta (concept: trombose van het valse lumen beschermt tegen expansie7,8)
- - Succes van stent-graft-plaatsing is 98% 4,6,7
- - 1-jaarsoverleving rond de 90% en de 3-jaarsoverleving tussen 75-85% 5,7,8
- Stanford type A
- - Bentall-procedure (aortaklep- en aorta ascendens vervanging + reimplantatie coronairen) 9
- Follow-up
- - Policontrole na 1, 3, 6 en 12 maanden, daarna jaarlijks
- - Follow-up beeldvorming middels MRI
- - Aandachtspunten: tekenen van aorta expansie, aneurysmaformatie, tekenen van lekkages op anastomoseplaatsen en stents, malperfusie
Complicaties
- Bij acute ongecompliceerde aortadissectie type B 7
- - Mortaliteit 40% in 1ste 3 maanden zonder behandeling
- - Mortaliteit 10-15% in 1ste jaar bij behandeling met bloeddrukverlagende middelen
- - Mortaliteit 30-50% na 5 jaar bij behandeling met bloeddrukverlagende middelen
- Bij aortadissectie type A
- - 15% mortaliteit bij chirurgie
- Bij endovasculaire stent-graft 10
- - Beroerte
- - Paraplegie
- - Verergering tot een aortadissectie Stanfordtype A
- - Darminfarcering
- - Noodzaak tot amputatie
Referenties
- 1. Olsson C, Thelin S, Stahle E, Ekbom A, Granath F. Thoracic aortic aneurysm and dissection: increasing prevalence and improved outcomes reported in a nationwide population-based study of more than 14,000 cases from 1987 to 2002. Circulation. 2006;114:2611-8.
- 2. Trimarchi S, Nienaber CA, Rampoldi V, Myrmel T, Suzuki T, Bossone E, et al. Role and results of surgery in acute type B aortic dissection: insights from the International Registry of Acute Aortic Dissection (IRAD). Circulation. 2006;114:I357-I64.
- 3. Daily PO, Truebold HW, Stinson EB, Wuerflein RD, Shumway NE. Management of acute aortic dissections. Ann Thorac Surg 1970;10:237-247
- 4. De Bakey ME, Henly WS, Cooley DA, Morris GC Jr, Crawford ES, Beall AC Jr. Surgical management of dissecting aneurysms of the aorta. J Thorac Cardiovasc Surg 1965;49:130-149
- 5. Eggebrecht H, Nienaber CA, Neuhauser M, Baumgart D, Kische S, Schmermund A, et al. Endovascular stent-graft placement in aortic dissection: a meta-analysis. Eur Heart J. 2006;27:489-98.
- 6. Nienaber CA, Zannetti S, Barbieri B, Kische S, Schareck W, Rehders TC. INvestigation of STEnt grafts in patients with type B Aortic Dissection: design of the INSTEAD trial--a prospective, multicenter, European randomized trial. Am Heart J. 2005;149:592-9.
- 7. Tsai TT, Fattori R, Trimarchi S, Isselbacher E, Myrmel T, Evangelista A, et al. Long-term survival in patients presenting with type B acute aortic dissection: insights from the International Registry of Acute Aortic Dissection. Circulation. 2006;114:2226-31.
- 8. Fattori R, Nienaber CA, Rousseau H, Beregi JP, Heijmen R, Grabenwoger M, et al. Results of endovascular repair of the thoracic aorta with the Talent Thoracic stent graft: the Talent Thoracic Retrospective Registry. J Thorac Cardiovasc Surg. 2006;132:332-9.
- 9. Bentall H., De Bono A. (1968). A technique for complete replacement of the ascending aorta. Thorax 23 (4): 338–9.
- 10. Rodriguez JA, Olsen DM, Lucas L, Wheatley G, Ramaiah V, Diethrich EB. Aortic remodeling after endografting of thoracoabdominal aortic dissection. J Vasc Surg. 2008;47:1188-94.