Atlanto-occipitale dislocatie
Atlanto-occipitale dislocatie
Auteur: J. Sprakel, MD - Laatste update: 21-12-2015
Atlanto-occipitale dislocatie

Oorzaak
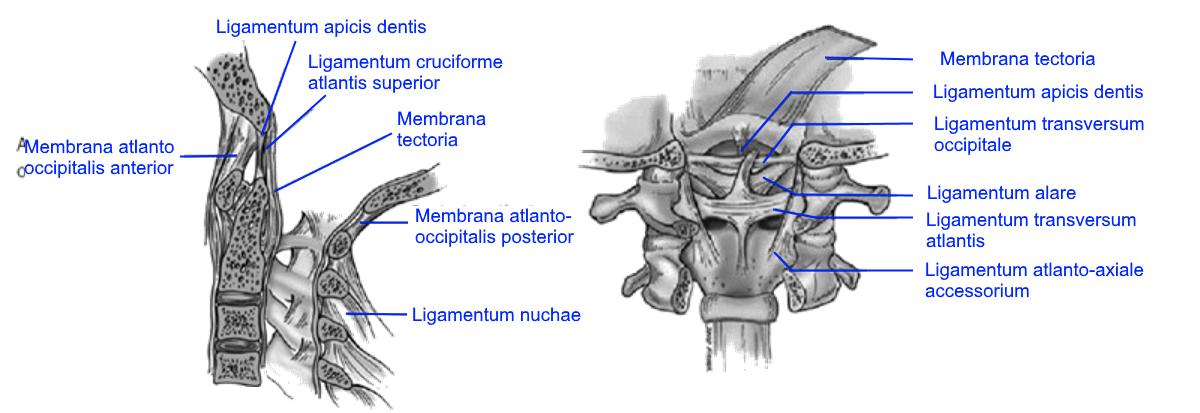
- - Ruptuur van ligamenten tussen schedel en bovenste cervicale wervels
- - Atlanto-occipitale dislocaties zijn meestal niet met het leven verenigbaar
- - 1% van alle cervicale letsels in acute setting
- - Vaak hoog-energetisch trauma (q. motorongelukken)
- - Komt 3x vaker voor bij kinderen en jong volwassenen (meer horizontaal gewrichtsoppervlak, relatief laxiteit van ligamentaire structuren en groot hoofd) 1
- - Zeldzaam letsel
Lichamelijk onderzoek
- - Soms asymptomatisch
- - Erge nekpijn
- - Spierzwakte
- - Apneu
- - Neurogene shock (autonome disregulatie)
- Neurologische uitvalsverschijnselen:
- - Lage craniale zenuw disfuncties (n. abducens, n. vagus en n. hypoglossus)
- - Unilaterale of bilaterale zwakte of zelfs quadriplegie
- - Hyperreflexie met clonus
- - Positieve Babinski
- - Abnormale sfinctertonus

Operatieve behandeling
Indicaties:- - Alle atlanto-occipitale dislocaties
(Na-)behandeling:
- - Harde nekkraag en spine-board
- - Consult neurochirurg
- - Zo snel mogelijk stabiliseren (reponeren) in halo-vest
- - Schedel (halo) tractie is gecontraïndiceerd (risico op 10% neurologische verslechtering) 4
- - Veelal is uiteindelijk chirurgische stabilisatie middels occipito-cervicale (C0-C2) artrodese noodzakelijk ter verkrijging van permanente stabiliteit danwel voorkoming van eventueel catastrofale reluxatie
Referenties
1. Bucholz RW, Burkhead WZ. The pathological anatomy of fatal atlanto-occipital dislocations. J Bone Joint Surg Am. 1979;61:248–250.2. Riascos R, Bonfante E, Cotes C et-al. Imaging of Atlanto-Occipital and Atlantoaxial Traumatic Injuries: What the Radiologist Needs to Know. Radiographics. 2015;35 (7): 2121-2134. doi:10.1148/rg.2015150035
3. Traynelis VC, Marano GD, Dunker RO, Kaufman HH. Traumatic atlanto-occipital dislocation. Case report. J Neurosurg. 1986;65:863–870
4. Theodore N, Aarabi B, Dhall SS, Gelb DE, Hurlbert RJ, Rozzelle CJ, Ryken TC, Walters BC, Hadley MN. The diagnosis and management of traumatic atlanto-occipital dislocation injuries. Neurosurgery. 2013;72 Suppl 2:114–126.
5. Nederlandse Orthopaedische Vereniging Richtlijn acute traumatische wervelletsels opvang, diagnostiek, classificatie en behandeling 2009