Geïsoleerde ulnaschachtfractuur
Geïsoleerde ulnaschachtfractuur
Auteur: J. Sprakel, MD - Laatste update: 15-04-2017
Geïsoleerde ulnaschachtfractuur

Diagnostiek
- Röntgenopnames
- - X-onderarm AP en lateraal (+ elleboog en pols op 1 plaat)
- Aandachtspunten
- - Angulatie
- - Ulnaire verkorting
- - Mate van dislocatie
| Mate van dislocatie volgens Altner en Hartman 1 | |
|---|---|
| Graad | Omschrijving |
| Niet gedisloceerd | |
| Enigszins gedisloceerd | Maximale verplaatsing dikte één cortex |
| Matig gedisloceerd | Verplaatsing 50% of meer diameter van het bot |
| Ernstig gedisloceerd | Geen botcontact tussen de fragmenten |
Classificatie
Classificatie volgens AO| Simpele fractuur | ||
|---|---|---|
| 22-A1 Ulna schachtfractuur, radius intact | ||
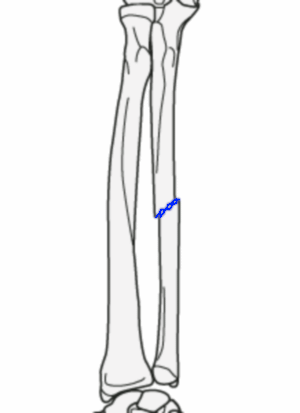
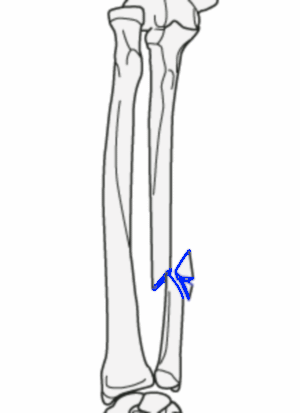
AO 22-A1.1 Schuine (of spiraal) schachtfractuur van de ulna |
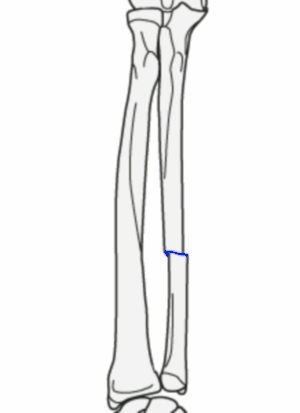
AO 22-A1.2 Dwarse schachtfractuur van de ulna |
AO 22-A1.3 Fractuur van de schachtfractuur met radiuskopluxatie (Monteggia) |
| Wedge (vlinderfragment) fractuur | ||
|---|---|---|
| 22-B1 Ulna schachtfractuur, radius intact | ||
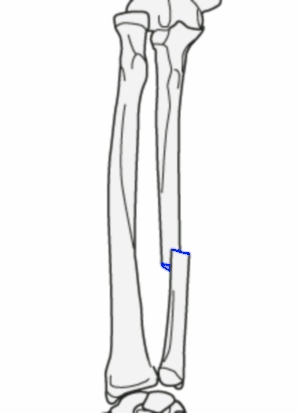
AO 22-B1.1 Ulna wedge fractuur |

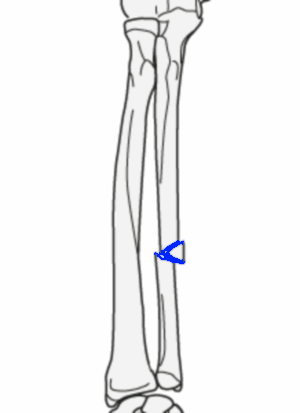
AO 22-B1.2 Multifragmentaire ulna wedge fractuur |
AO 22-B1.3 Ulna wedge fractuur met radiuskopluxatie (Monteggia) |
| Complexe fractuur | ||
|---|---|---|
| 22-C1 Bifocaal ulna schachtfractuur, radius intact | ||
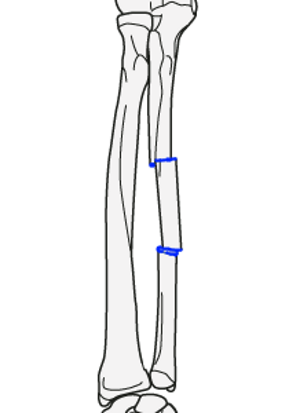
AO 22-C1.1 Bifocaal ulnaschachtfractuur |
||
Conservatieve behandeling
Indicaties:- - Niet gedisloceerde fracturen 2-4
- - Enigszins gedisloceerde geïsoleerde ulnaschachtfracturen (stabiel) 2-4
- - schachtdislocatie <25-50% 3,5-8
- - angulatie in elk vlak van <8o 3, 9-10
(Na-)behandeling:
- - 4-6 weken onderarmgips (geen bovenarmgips) 11,12-13
- - 6 weken onbelast
- - Direct X-controle in gips (aandacht voor stand elleboog en pols)
Follow-up:
-
Poliklinische follow‐up Na 1 week Na 6 weken Na 3 maanden Na 6 maanden (op indicatie) - X-onderarm
- Gipswissel naar kunsstof- Gips af
- X-onderarm
- Oefeninstructies
- Fysiotherapie op indicatie- Functiecontrole
- X-onderarm- Op indicatie bij klachten
- Aandachtspunten klinische follow-up:
- - Functionele classificatie volgens Zych
- - Pijn in rust en bij activiteit (aanwezig of afwezig)
- - Knijpkracht (volledig hersteld, iets verlaagd, matig verminderd (de helft van normaal) of ernstig verminderde)
- - Type van werk en level van activiteit (pre-trauma, sommmige veranderingen of werkrestricties, heeft activiteiten of werk niet kunnen te hervatten)
Functionele classificatie volgens Zych 14 Graad Omschrijving Excellent - Geen pijn
- >90% normale onderarm rotatie en beweging in elleboog, pols en handGoed - Milde pijn bij forse inspanning
- 70%-90% normale onderarm rotatie en beweging in elleboog, pols en handSlecht - Matige tot ernstige pijn
- <70% normale onderarm rotatie en beweging in elleboog, pols en hand
- Aandachtspunten radiologische follow-up:
- - Axiale angulatie <8o
- - Verkorting <2mm
- - Dislocatie <25-50%
Operatieve behandeling
Indicaties:- - Matig of ernstig gedisloceerde geïsoleerde ulnaschachtfracturen (instabiel)2-3
- - schachtdislocatie >25-50% 3,5-8
- - angulatie in elk vlak van >8o 3,9-10
(Na-)behandeling:
(Na-)behandeling:
- - 2 weken gips voor wondgenezing
- - Vanaf 2de week oefenen, eventueel onder fysiotherapeutische begeleiding
- - VOSM op indicatie, pas na 1 - 1,5 jaar (in dagbehandeling) 15
Follow-up:
-
Poliklinische follow‐up Na 2 weken Na 6 weken Na 3 maanden Na 6 maanden (op indicatie) - Gips af
- Oefeninstructies
- Evt. fysiotherapie- Functiecontrole
- X-onderarm
- Fysiotherapie op indicatie- Functiecontrole
- X-onderarm
- Fysiotherapie op indicatie- Op indicatie bij klachten
- Aandachtspunten klinische follow-up:
- - Functionele classificatie volgens Zych
- - Pijn in rust en bij activiteit (aanwezig of afwezig)
- - Knijpkracht (volledig hersteld, iets verlaagd, matig verminderd (de helft van normaal) of ernstig verminderde)
- - Type van werk en level van activiteit (pre-trauma, sommmige veranderingen of werkrestricties, heeft activiteiten of werk niet kunnen te hervatten)
Functionele classificatie volgens Zych 14 Graad Omschrijving Excellent - Geen pijn
- >90% normale onderarm rotatie en beweging in elleboog, pols en handGoed - Milde pijn bij forse inspanning
- 70%-90% normale onderarm rotatie en beweging in elleboog, pols en handSlecht - Matige tot ernstige pijn
- <70% normale onderarm rotatie en beweging in elleboog, pols en hand
- Aandachtspunten radiologische follow-up:
- - Axiale angulatie <8o
- - Verkorting <2mm
- - Dislocatie <25-50%
Complicaties
- Conservatieve behandeling:10
- - Pijn
- - Beperkingen in Range of Motion (4-35%) 3,5-7,10,16,17-21
- - Delayed union (27.3%)
- - Malunion (angulatie van >10o aan einde van follow-up) (45.5 %)22
- - Nonunion (36.4%)
- - Secundaire dislocatie (30.3%)
- - Gipsklachten (12.1%)
- Zeldzaam:
- - DVT
- - Zenuwletsel
- - Refractuur
- - Radio-ulnaire synostose 23
- - Heterotope ossificaties
- - CRPS
- - Compartiment syndroom
- Operatieve behandeling:10
- - Pijn
- - Beperkingen in Range of Motion (2-35%)10,20,24-28
- - Delayed union (21.6%)
- - Malunion (angulatie van >10o aan einde van follow-up) (5,4%)22
- - Nonunion (5.4%)
- - Secundaire dislocatie (2.7%)
- - Materiaalfalen (8.1%)
- - Wondinfectie(5.4%)
- - Uitbreken osteosynthesemateriaal (5.4%)
- - Voelen van / verwijderen osteosynthesemateriaal (24.3%)
- Zeldzaam:
- - DVT
- - Zenuwletsel
- - Refractuur
- - Radio-ulnaire synostose 23
- - Heterotope ossificaties
- - CRPS
- - Compartiment syndroom


Referenties
- 1. Altner PC, Hartman JT (1972) Isolated fractures of the ulnar shaft in the adult. Surg Clin North Am 52:155-170
- 2. Van Leemput T, Mahieu G. Conservative management of minimally displaced isolated fractures of the ulnar shaft. Acta Orthop Belg 2007;73:710–3.
- 3. Zych GA, Latta LL, Zagorski JB. Treatment of isolated ulnar shaft fractures with prefabricated functional fracture braces. Clin Orthop Relat Res 1987;194–200.
- 4. Gebuhr P, Hölmich P, Orsnes T, Soelberg M, Krasheninnikoff M, Kjersgaard AG. Isolated ulnar shaft fractures. Comparison of treatment by a functional brace and long-arm cast. J Bone Joint Surg Br. 1992 Sep;74(5):757-9.
- 5. Dymond IW. The treatment of isolated fractures of the distal ulna. J Bone Joint Surg Br 1984;66:408–10.
- 6. Ekkernkamp A, Muhr G. Stable fracture of the ulna shaft. Biomechanics and therapeutic consequences. Unfallchirurg 1988;91:551–6.
- 7. Corea JR, Brakenbury PH, Blakemore ME. The treatment of isolated fractures of the ulnar shaft in adults. Injury 1981;12:365–70.
- 8. Szabo RM, Skinner M. Isolated ulnar shaft fractures. Retrospective study of 46 cases. Acta Orthop Scand 1990;61:350–2.
- 9. Sauder DJ, Athwal GS. Management of isolated ulnar shaft fractures. Hand Clin 2007;23:179–84. vi.
- 10. Marlon O. Coulibaly, Clifford B. Jones, Debra L. Sietsema, Thomas A. Schildhauer Results of 70 consecutive ulnar nightstick fractures Injury, Int. J. Care Injured 46 (2015) 1359–1366
- 11. Brakenbury PH, Corea JR, Blakemore ME. Non-union of the isolated fracture of the ulnar shaft in adults. Injury 1981;12:371–5.
- 12. Handoll HH, Pearce P. Interventions for isolated diaphyseal fractures of the ulna in adults. Cochrane Database Syst Rev 2009;(3):CD000523.
- 13. Mackay D, Wood L, Rangan A. The treatment of isolated ulnar fractures in adults: a systematic review. Injury. 2000 Oct;31(8):565-70.
- 14. Zych GA, Latta LL et al (1987) Treatment of isolated ulnar shaft fractures with prefabricated functional fractures braces. Clin Orthop 219 : 194-200
- 16. Pollock FH, Pankovich AM, Prieto JJ, Lorenz M. The isolated fracture of the ulnar shaft. Treatment without immobilization. J Bone Joint Surg Am 1983;65:339–42.
- 17. Ostermann PA, Ekkernkamp A, Henry SL, Muhr G. Bracing of stable shaft fractures of the ulna. J Orthop Trauma 1994;8:245–8.
- 18. Hackstock H, Helmreich M. Isolated fractures of the ulnar shaft. Treatment with the Sarmiento brace. Unfallchirurg 1987;90:298–302.
- 19. Sarmiento A, Latta LL, Zych G, McKeever P, Zagorski JP. Isolated ulnar shaft fractures treated with functional braces. J Orthop Trauma 1998;12:420–3
- 20. Hooper G. Isolated fractures of the shaft of the ulna. Injury 1974;6:180–4.
- 21. Goel SC, Raj KB, Srivastava TP. Isolated fractures of the ulnar shaft. Injury 1991;22:212–4.
- 22. Tarr RR, Garfinkel AI, Sarmiento A. The effects of angular and rotational deformities of both bones of the forearm. An in vitro study. J Bone Joint Surg Am 1984;66:65–70.
- 23. Watson FM Jr, Eaton RG (1978) Post-traumatic radio-ulnar synostosis. J Trauma 18:467-468
- 24. Anderson LD, Sisk D, Tooms RE, Park III WI. Compression-plate fixation in acute diaphyseal fractures of the radius and ulna. J Bone Joint Surg Am 1975;57:287–97.
- 25. Boussouga M, Bousselmame N, Lazrek K, Taobane H. Surgical management of isolated fractures of the ulnar shaft. Acta Orthop Belg 2002;68:343–7.
- 26. Leung F, Chow SP. A prospective, randomized trial comparing the limited contact dynamic compression plate with the point contact fixator for forearm fractures. J Bone Joint Surg Am 2003;85-A:2343–8.
- 27. Chapman MW, Gordon JE, Zissimos AG. Compression-plate fixation of acute fractures of the diaphyses of the radius and ulna. J Bone Joint Surg Am 1989;71:159–69
- 28. Grace TG, Eversmann Jr WW. Forearm fractures: treatment by rigid fixation with early motion. J Bone Joint Surg Am 1980;62:433–8.